Welcome to the CountyCare Provider Network
Thank you for being a part of the CountyCare provider network. We’re excited to be your partner as we work together to improve the health of our members.
Questions? We're here to help!
Email us at: [email protected]
Call us at: 312-864-8200 / 855-444-1661 (toll-free) / 711 (TDD/TTY)
Monday-Friday, 8am-5pm CST
Quick Links

Provider Roster Training Events
Prior Authorizations
Some services require prior authorization for reimbursement to be issued to the provider. All out-of-network and out-of-state services require prior authorization except for Emergency Care and Family Planning Services.
Prior Authorization Look-up Tool
Check PA requirements instantly
Clinical Criteria for Prior Authorization
Review approval criteria
Medical Drug Policies for Prior Authorization
Access drug PA policies
Questions? View our FAQs or call the CountyCare Medical Management and Prior Authorization Department at 312-864-8200 / 855-444-1661.
Prior Authorization for Statistical Data
Prior Authorization for Medical and Behavioral Health Services
For efficiency and easier tracking, submit your Medical Prior Authorization request through the CountyCare Provider Portal.
You can also submit prior authorization requests via fax using these forms:
Prior Authorization for Musculoskeletal Services
Including musculoskeletal surgery for the spine, interventional pain management (IPM), physical, occupational and speech therapy, advanced imaging and diagnostic cardiology services
Submit to: Evolent Specialty Services (formerly National Imaging Associates)
Prior Authorization for Cardiology Services
Including oncology, imaging, radiology and oncology medication, cardiology medication, and hospital review services
Submit to: Evolent Specialty Services (formerly New Century Health)
Prior Authorization for Maternity Services
Including maternity and NICU care management services
Submit to: Progeny Health
Prior Authorization for Prescription Drug Services
CountyCare maintains a Preferred Drug List (PDL), the same PDL as Illinois Medicaid and all Medicaid Health Plans in Illinois. The CountyCare PDL includes a wide variety of generic and brand name drugs. Clinicians are encouraged to prescribe from the CountyCare PDL for their patients who are members of CountyCare.
CountyCare works with CVS Caremark to administer pharmacy benefits, including the pharmacy prior authorization process. CountyCare requires prior authorization for select drugs on the PDL as well as ALL drugs not on the PDL. The PDL indicates which drugs require prior authorization. Most specialty drugs are not on the PDL and require prior authorization as described below.
Follow these steps for efficient processing of your pharmacy prior authorization requests:
- Complete the CVS Caremark: Medication Request Form or Universal PA Form. Include detailed clinical information that will help CVS Caremark understand the need for the drug being requested.
- Fax to CVS Caremark at 1-866-255-7569.
- Once approved, CVS Caremark notifies the prescriber by fax and member by letter.
- For urgent or after-hours requests, a pharmacy can provide up to a 72-hour supply of most medications by calling the CVS Caremark Pharmacy Help Desk at: 1-800-364-6331.
Submit all completed forms to CVS Caremark
Prior Authorization for Specialty Pharmacy Services
To submit a specialty pharmacy prior authorization, complete the Medication Request Form.
Fax all completed forms to CVS Caremark: 1-866-255-7569
Prior Authorization for Dental and Vision Services
Submit dental and vision prior authorization through the Avesis portal or by calling 866-337-1594.
Phone: 866-337-1594
Provider Billing Resources
Illinois Association of Medicaid Health Plans (IAMHP) and its member plans have developed a comprehensive billing manual to better assist providers. We encourage you to reference it for specific billing information.
IAMHP Billing Manual
Comprehensive guide for provider billing
Claim Projects
Review Claims & Configurations issue logs
CountyCare Claim Remark Code Look-Up
Search and understand claim codes
Claims Processing
CountyCare has partnered with Evolent Health to process claims. Claims eligible for payment must meet the following requirements:
- The member is effective with CountyCare Health Plan on the date of service
- The service provided is a covered benefit under the member’s contract on the date of service
- Referral and prior authorization processes were followed, if applicable
- Claim was received within 180 calendar days from the date of service, or date of discharge, whichever is later. This limit may be extended where eligibility has been retroactively received by CountyCare up to a maximum of 180 days.
- Corrected claims must be submitted within 60 days of the explanation of payment (EOP), or 180 days from the date of service, whichever is later.
Providers have the right to request a review of any claim decision made by CountyCare within 60 calendar days from the date of the explanation of payment (EOP) or Remittance Notice. Provider claim reviews may be submitted electronically through the Provider Portal or by mail using the Claim Review form for any of the following denial reasons: timely filing, review of contract rate/payment, duplicate claim, authorization, or other unforeseen reason.
For more detailed information on claims submission and adjudication, please view the Provider Manual.
Electronic Transactions and Electronic Remittance Advice
Network providers are encouraged to participate in CountyCare’s electronic claims/encounter filing program. You or your billing agent will need to utilize a third-party claims clearinghouse vendor to submit electronic claims. CountyCare can receive ANSI X12N 837, or most current version, professional, institution or encounter transactions. In addition, it can generate an ANSI X12N 835, or most current version electronic remittance advice known as an Explanation of Payment (EOP).
Providers that bill electronically have the same timely filing requirements as providers filing paper claims. In addition, providers that bill electronically must monitor their error reports and evidence of payments to ensure all submitted claims and encounters appear on the reports. Providers are responsible for correcting any errors and resubmitting the affiliated claims and encounters.
CountyCare provides Electronic Funds Transfer (EFT) and Electronic Remittance Advice (ERA) electronic remittance advice known as an Explanation of Payment (EOP) to its participating providers via Instamed to help them reduce costs, speed secondary billings, and improve cash flow by enabling online access to remittance information, and straightforward reconciliation of payments.
Visit Instamed to register:
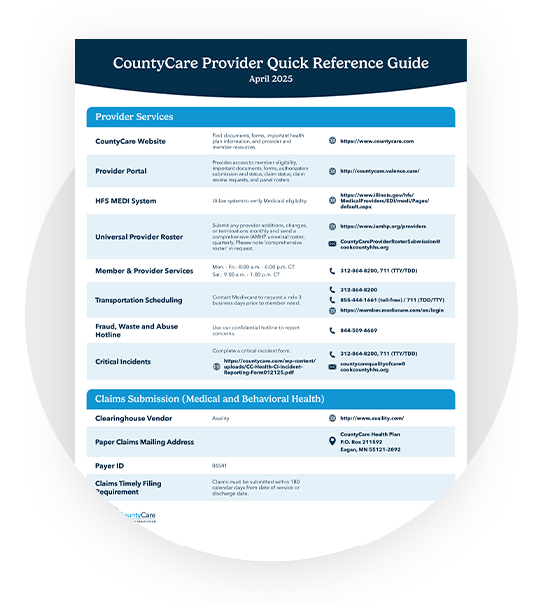
CountyCare’s Payor ID is: 06541.
CountyCare’s Clearinghouse vendor is Availity.
Claim Projects
Please review the reports below for details around current or recently completed Claims and Configuration projects from CountyCare. The report outlines project description, impacted providers, expected resolution, current status, and expected completion date, when known. If you have any questions about the projects on this report, please contact your Provider Relations Representative.
CountyCare Claims – Configuration Project Updates 07-21-2026
CountyCare Claims – Configuration Project Updates 06-23-2026
CountyCare Claims – Configuration Project Updates 06-09-2026
CountyCare Claims – Configuration Project Updates 05-29-2026
Healthcare and Family Services (HFS) Billing Resources
Rates and Fee Schedules:
HFS Provider Handbooks:
HFS Provider Notices:
Clinical Practice Guidelines
Preventative Health Guidelines & Minimum Standards of Care
Medically Necessary Services
- CountyCare providers are expected to provide any further medically necessary diagnostic study or treatment for any known condition or conditions discovered during the complete health history and physical examination if the study or treatment is within the scope of covered services
- Any condition discovered during the screening examination or screening test requiring further diagnostic study or treatment must be provided if within the scope of Covered
- If a condition is discovered that requires treatment outside the scope of service, the provider should refer to an appropriate source of care and may look to CountyCare to assist with such referral.
Specialty Care Services
- CountyCare provides for a full range of specialty care services within the scope of covered services.
- Primary care clinicians are expected to refer members to CountyCare network specialists, as medically appropriate, when managing the healthcare needs of members beyond the primary clinician’s training and knowledge.
- Specialists may also refer to other specialists, as appropriate, in consultation with the member’s primary care clinician.
- CountyCare will assist in identifying available specialists through our case management program. Case managers may be identified by calling Member Services at 312-864-8200.
Barriers or Restrictions to Access to Care
CountyCare is committed to key principles of access to healthcare: affordability, accommodation, availability, accessibility, and acceptability. In its use of utilization management methods, such as prior authorizations or step-failure therapy requirements, CountyCare does not present barriers or restrictions to access to care for medically necessary services. CountyCare covers and offers all FDA-approved birth control methods with education and counseling on the most effective methods first, specifically long-acting reversible contraception (LARC). Enrollees have the freedom to choose the preferred birth control method that is most appropriate for them.
Clinical Practice Guidelines
All services coordinated by CountyCare must be in accordance with established evidence-based best practice standards of care. Clinical practice guidelines are intended to optimize our members care, and are adopted in consultation with CountyCare Network Providers.
Guidelines are reviewed no less than biennially or in timely response to changes in best practice. For questions or comments, providers may email [email protected].
Clinical Practice Guidelines
Adult Preventive Care
Acute Respiratory Distress Syndrome (ARDS)
Adult Behavioral Health
- American Psychiatric Association: Psychiatric Evaluation of Adults**
- American Psychiatric Association: Acute Stress Disorder and PTSD**
- American Psychiatric Association: Major Depressive Disorder**
- American Psychiatric Association: Obsessive-Compulsive Disorder**
- American Psychiatric Association: Substance Use**
- **Please press cancel at the login page
- SAMHSA: Family-Centered Treatment for Women with Substance Abuse Disorders
- Opioid Use and Opioid Use Disorder in Pregnancy | ACOG
Asthma
Bronchitis
Cancer
Cardiovascular Disease and Congestive Heart Failure
Chronic Kidney Disease
Chronic Obstructive Pulmonary Disease
Clinical Pharmacy Medication Review
Community Reintegration
Coronary Artery Disease
- American Heart Association & American College of Cardiology (link works best in Internet Explorer browser)
Coronavirus
Dental Services
Diabetes
Human Immunodeficiency Virus (HIV)
Long-term Supports & Services (LTSS
Low Back Pain
Myocardial Infarction
Pain Management
Pediatric Behavioral Health
- American Academy of Child & Adolescent Psychiatry: Psychotropic Medication
- American Academy of Child & Adolescent Psychiatry: Autism Spectrum
- American Academy of Pediatrics: Attention Deficit Hyperactivity Disorder
- American Academy of Child & Adolescent Psychiatry: Obsessive-Compulsive Disorder
- American Academy of Child & Adolescent Psychiatry: Cultural Competence
Pediatric Preventive Care
Psychotropic Medication Management
Seizure Disorder
Respiratory Syncytial Virus (RSV)
Reproductive Health Care
Stroke
Smoking Cessation
Special Needs Children
Preventative Health Guidelines
All CountyCare network providers should follow the preventative health guidelines outlined below by Illinois Healthcare and Family Services.
Preventive Health Guidelines and Minimum Standards of Care
CountyCare providers must adhere to minimum standards of care as outlined in the following guidelines: https://countycare.com/wp-content/uploads/GuidelinesforPerinatalCare-7thed.pdf
Medically Necessary Services
- CountyCare providers are expected to provide any further medically necessary diagnostic study or treatment for any known condition or conditions discovered during the complete health history and physical examination if the study or treatment is within the scope of covered services
- Any condition discovered during the screening examination or screening test requiring further diagnostic study or treatment must be provided if within the scope of Covered Services.
- If a condition is discovered that requires treatment outside the scope of service, the provider should refer to an appropriate source of care and may look to CountyCare to assist with such referral.
Specialty Care Services
- CountyCare provides for a full range of specialty care services within the scope of covered services.
- Primary care clinicians are expected to refer members to CountyCare network specialists, as medically appropriate, when managing the healthcare needs of members beyond the primary clinician’s training and knowledge.
- Specialists may also refer to other specialists, as appropriate, in consultation with the member’s primary care clinician.
- CountyCare will assist in identifying available specialists through our case management program. Case managers may be identified by calling Member Services at 312-864-8200.
Adult: General
CountyCare expects that a complete health history and physical examination1 is provided to each member initially within the first year of enrollment and every 1-3 years thereafter, or as indicated by need and clinical care guidelines. For those aged 65 and older, a complete health history and physical examination should be conducted annually. With each health history and physical examination, screening, counseling, and immunization should be provided in accordance with national medical organizations’ guidelines.
1For purposes of this section, a “complete health history and physical examination” shall include, at a minimum, the following health services regardless of age and gender of each Enrollee
- Initial and interval history, including past medical and surgical history of each Enrollee, history of allergies, an updated list of medications used (prescribed and over the counter), and a family medical history.
- Height and weight measurement for body mass index (BMI).
- Blood pressure, temperature, and pulse rate measurements.
- Nutrition and physical activity assessment and counseling.
- Assessment of social and economic determinants of health; housing, transportation availability, and employment
- Screening for alcohol, tobacco, substance abuse, intimate partner violence, and depression screening and counseling.
- Counseling for advanced directives (living will and healthcare power of attorney) and collection of those documents, if available.
- Verification of contact information for medical follow up when necessary such as postal address, e-mail, and phone number (landline, mobile, and alternate number for a family member if unable to reach patient directly); and
- Health promotion and anticipatory guidance, as clinically appropriate.
Pediatric: General
CountyCare expects that a complete health history and physical examination is provided to each member per the following schedule from Illinois Healthcare and Family Services guidelines:
Age Group | Schedule |
|---|---|
Under Age One | Within 24 hours of birth in hospital, 3-5 days of life and within 48-72 hours after discharge, 1 month, 2 months, 4 months, 6 months, 9 months |
Age 1-3 | 12 months, 15 months, 18 months, 24 months, 30 months |
Age 3-21 | Annually, per provider |
Pediatric: EPSDT
CountyCare providers are expected to employ strategies to ensure that children receive comprehensive child EPSDT health services as needed in in conformance with the Handbook for Providers of Healthy Kids Services, which can be found at Illinois Healthcare and Family Services.
Cervical Cancer Screening
**Recommendation is currently being updated by US Preventive Services Task Force
The USPSTF recommends screening for cervical cancer every 3 years with cervical cytology alone in women aged 21 to 29 years. For women aged 30 to 65 years, the USPSTF recommends screening every 3 years with cervical cytology alone, every 5 years with high-risk human papillomavirus (hrHPV) testing alone, or every 5 years with hrHPV testing in combination with cytology (cotesting).
Breast Cancer Screening
Women aged 40 to 74 are recommended to have biennial mammogram screenings. Clinical breast exams are recommended every one (1) to three (3) years from 20 to 40 years old and annually thereafter. Breast self-awareness to recognize changes can be discussed from age 20 years old. Using one of several tools, women with a family history of breast, ovarian, tubal, or peritoneal cancer should be offered the gene mutation screening for BRCA1 and BRCA2. Subsequent positive testing should be offered genetic counseling. Women who are at increased risk for breast cancer should be counseled and offered risk reducing medication such as selective estrogen response modulators
Colorectal Cancer Screening
Routine screening recommended for Persons 45-75 years of age. Screening intervals and strategies include the following:
- High-sensitivity guaiac fecal occult blood test (HSgFOBT) or fecal immunochemical test (FIT) every year
- Stool DNA-FIT every 1 to 3 years
- Computed tomography colonography every 5 years
- Flexible sigmoidoscopy every 5 years
- Flexible sigmoidoscopy every 10 years + annual FIT
- Colonoscopy screening every 10 years
Lung Cancer Screening
The USPSTF recommends annual screening for lung cancer with low-dose computed tomography (LDCT) in adults aged 50 to 80 years who have a 20 pack-year smoking history and currently smoke or have quit within the past 15 years. Screening should be discontinued once a person has not smoked for 15 years or develops a health problem that substantially limits life expectancy or the ability or willingness to have curative lung surgery.
Prostate Cancer Screening
The discussion about screening should take place at:
- Age 50 for men who are at average risk of prostate cancer and are expected to live at least 10 more years
- Age 45 for men at high risk of developing prostate cancer. This includes African American men and men who have a first-degree relative (father or brother) diagnosed with prostate cancer at an early age (younger than age 65).
- Age 40 for men at even higher risk (those with more than one first-degree relative who had prostate cancer at an early age)
Skin Cancer Screening
The US Preventive Services Task Force has concluded that the current evidence is insufficient and that the balance of benefit and harms of visual skin by a clinician to screen for skin cancer in asymptomatic adults cannot be determined.
Diabetes Mellitus Type 2 Screening
The USPSTF recommends screening for abnormal blood glucose as part of cardiovascular risk assessment in adults aged 35 to 70 years who are overweight or obese. Clinicians should offer or refer patients with abnormal blood glucose to intensive behavioral counseling interventions to promote a healthful diet and physical activity.
Lipid Disorder Screening
For adults aged 40 to 75 years who have 1 or more cardiovascular risk factors and an estimated 10-year cardiovascular disease (CVD) risk of 10% or greater, The USPSTF recommends that clinicians prescribe a statin for the primary prevention of CVD for adults aged 40 to 75 years who have 1 or more CVD risk factors (i.e. dyslipidemia, diabetes, hypertension, or smoking) and an estimated 10-year risk of a cardiovascular event of 10% or greater.
Pediatric: US Preventive Services Task Force has concluded that the current evidence is insufficient to assess the balance of benefits and harms of screening for lipid disorders in children and adolescents 20 years or younger.
Hepatitis C Screening
The USPSTF recommends screening for hepatitis C virus (HCV) infection in adults aged 18 to 79 years.
Osteoporosis Screening
Screen women 65 years or older with dual energy x-ray absorptiometry (DXA) bone mineral density (BMD), with or without fracture risk assessment. For postmenopausal women younger than 65 years with 1 or more risk factors, screening may begin earlier. Risk factors may include certain ethnicities, very low BMI, history of fractures, tobacco use, limited exercise, and other chronic diseases.
Tuberculosis Screening
Screening for latent tuberculosis infection is recommended for all at risk enrollees. At risk may include signs and symptoms of tuberculosis, recent contact with someone diagnosed with tuberculosis, occupational or living hazard of close quarters (congregate setting), and recent immigrants from county with high prevalence of tuberculosis, compromised immune system, or healthcare workers.
Immunizations: Age & Interval Recommendations
**Recommendation is currently being updated by US Preventive Services Task Force
The following are recommended immunizations by age and interval for both males and females, unless contraindicated:
- Influenza: One (1) dose annually
- Tetanus/ Diphtheria (Tdap/Td): One Tdap and one Td booster every ten (10) years
- Varicella: One (1) two dose series for all adults without previous evidence of immunity
- Human Papilloma Virus (HPV): 2 or 3 doses depending on age at initial vaccination or condition
- Shingles (Zoster): One (1) dose at 50 years of age and older
- Hepatitis A & B: combined Hepatitis A and Hepatitis B one (1) three dose series or Hepatitis A one (1) two dose series or Hepatitis B one (1) three dose series provided at any age for any Enrollee requesting protection.
- Covid 19:
- Children
- All children ages 6 months through 23 months.
- Children ages 2 years through 17 years in the following risk categories (Self-attestation of risk by the parent/guardian is acceptable.):
- Persons at high risk of severe COVID-19 (see Appendix C)
- Residents of long-term care facilities or other congregate settings
- Persons who have never been vaccinated against COVID-19
- Persons whose household contacts are at high risk for severe COVID-19.
- Children ages 2 years through 17 years based on shared clinical decision-making if not included in a risk group but whose parent or guardian desires their protection from COVID-19.
- Pregnant People
- All individuals who are or will be pregnant, during any trimester of pregnancy, postpartum, or during lactation.
- Adults
- All adults ages 18 years and older.
- RSV:
- One (1) dose RSV Vaccine (Abrysvo) for pregnant members at 32 weeks gestation through 36 weeks 6 days gestation from September through January, regardless of previous RSV infection.
- One (1) dose of RSV Vaccine (Niresvimab-Beyfortus) within one week of birth in hospital or outpatient setting for Infants born October-March whose mother did not receive RSV vaccine OR mother’s RSV vaccination status is unknown OR Mother received RSV vaccine less than 14 days prior to delivery.
- One (1) dose of RSV Vaccine (Niresvimab-Beyfortus) before the start of RSV season for infants born April-September whose mother did not receive RSV vaccine OR mother’s RSV vaccine stats us unknown OR whose mother received RSV vaccine less than 14 days prior to delivery.
- Inactivated poliovirus: One (1) 4-dose series at ages 2, 4, 6–18 months, 4–6 years; administer the final dose on or after age 4 years and at least 6 months after the previous dose.
- Adults known or suspected to be unvaccinated or incompletely vaccinated: administer remaining doses (1, 2, or 3 IPV doses) to complete a 3-dose primary series. (Complete primary series consists of at least 3 doses of IPV or trivalent oral poliovirus vaccine (tOPV) in any combination.)
**Please use the links above to visit the CDC website for Special Situations, Contraindications and precautions, more periodicity schedules, and vaccines specific to adults and children
Family Planning & Reproductive Health Care
Centers for Disease Control & Prevention
Recommendations for Contraceptive Use
American Society for Colposcopy & Cervical Pathology
- The full spectrum of family planning options and reproductive health services shall be appropriately provided within the Provider’s scope of practice and competence. The family planning and reproductive health services are defined as those services offered, arranged, or furnished for the purpose of preventing an unintended pregnancy, or to improve maternal health and birth outcomes. Standards of care and guidelines comply with the requirements of the Affordable Care Act. Federal and State laws regarding minor consents and confidentiality will be followed.
- Education and counseling on all contraceptive methods with emphasis on presenting the most effective methods first, specifically long-acting reversible contraceptives (LARC) such as intrauterine devices (IUD) and the implantable rod.
- Reproductive Life Plan which may include a preconception care risk assessment and preconception and interconception care discussions
- Education and Counseling on all contraceptive methods with emphasis on presenting the most effective methods first, specifically long-acting reversible contraceptives (LARC) such as intrauterine devices (IUD) and the implantable rod
- Emergency Contraception methods must include over-the-counter and prescription emergency contraception as well as the provision of the copper IUD for emergency contraception
- Permanent Methods of Birth Control: tubal ligation, transcervical sterilization and vasectomy
- Basic Infertility Counseling consisting of medical/sexual history review and fertility awareness education. Infertility medications and procedures are NOT covered
- Reproductive Health Exam with pelvic exam decoupled from the provision of contraception
- Sexually Transmitted Infections
- < 26 y/o Sexually Active Females & Males should be screened annually for chlamydia and gonorrhea.
- All Enrollees > 26 y/o should be screened based on risk factors (symptoms, new partner, multiple partners, or recent history of another STI)
- Universal HIV Testing, Counseling & Screening
- Testing & Treatment for genital and related infections, and other pathological conditions
- Lab Testing necessary for family planning and reproductive health services
- Cervical Cancer Screening, Management, and Early Treatment
- Vaccines for Preventable Reproductive Health Related Conditions, such as HPV and Hepatitis B
- Mammography Referral and BRCA Genetic Counseling & Testing
Barriers or Restrictions to Access to Care
CountyCare is committed to key principles of access to healthcare: affordability, accommodation, availability, accessibility, and acceptability. In its use of utilization management methods, such as prior authorizations or step-failure therapy requirements, CountyCare does not present barriers or restrictions to access to care for medically necessary services. CountyCare covers and offers all FDA-approved birth control methods with education and counseling on the most effective methods first, specifically long–acting reversible contraception (LARC). Enrollees have the freedom to choose the preferred birth control method that is most appropriate for them.
Maternity Care
Maternity Care
Prenatal Evaluation
A comprehensive prenatal evaluation and care in accordance with the latest standards as recommended by the American College of Obstetricians and Gynecology or the American Academy of Family Physicians, including ongoing risk assessment and development of individualized care plans that take into consideration the medical, psychosocial, cultural/linguistic, and educational needs of the patient and her family.
Systems & Protocols
Providers shall have systems and protocols in place to handle regular appointments, early entry to care appointments, after hours care with emergency appointment slots, seamless process for transmitting prenatal records to the delivering facility, and a referral network for mental health, social services, and specialty care. All pregnant women must be referred to the Women, Infants and Children’s (WIC) Supplemental Nutrition Program and have or be linked to case management services for identified high risk Enrollees. Providers shall be able to provide equal, high quality obstetrical care to special populations such as adolescent, homeless, developmentally, and intellectually disabled pregnant patients.
Prenatal Care
- Risk Counseling for STI/HIV, intimate partner violence, teratogen exposure, substance use and abuse and potential for pre-term delivery screenings, and education on use of 17 P, if appropriate.
- Screening For, Diagnosing, And Treating Depression before, during and after pregnancy with any number of tested screening tools (refer to the Healthy Kids Handbook for a list of approved screening tools).
- Health Maintenance promotion includes nutrition, exercise, dental care, immunizations, management of current chronic disease, over the counter and prescription medication, breastfeeding counseling and recommendation, appropriate weight gain in pregnancy, obesity counseling, managing signs and symptoms of common pregnancy ailments, and referral to breastfeeding, childbirth classes, and text4baby. The influenza vaccine should be offered to all pregnant women during influenza season regardless of gestational age. Tdap should be provided regardless of prior interval of Td or Tdap.
- Routine Laboratory Screening and Physical Exam, which includes dating by ultrasound for accurate gestational age. Every prenatal exam at minimum should include blood pressure check, fetal growth assessment, and fetal heart rate check. In the absence of patient symptoms and/or suspicion for preeclampsia, renal disease, or urinary tract infection, a urine analysis and culture is only required at the initial visit. Routine laboratory screening should include the following: blood type, Rh type, antibody, CBC (routine screening for anemia), rubella, hepatitis B, syphilis/gonorrhea/chlamydia/HIV, varicella, diabetes, and tuberculosis to applicable populations.
- Genetic Screening should be counseled and offered depending on patient’s age, medical/ family history, and ethnic background.
- Visit Protocols. Visits approximate to the third trimester should include labor preparation, education regarding preeclampsia, warning signs of miscarriage, fetal movements/kick count, preterm labor and labor, options for intrapartum care, breastfeeding encouragement, postpartum family planning including LARC or permanent sterilization with informed consent done prior to labor and delivery, circumcision, newborn provider care, car seat, SIDS, the importance of waiting at least 39 weeks to deliver, referral to parenting classes and WIC, and transition of maternal healthcare after the postpartum visit, as well as protocols to facilitate the continuum of care after the obstetric period.
Identify High-Risk Pregnancies
All Providers are required to timely identify high-risk pregnancies and arrange for maternal fetal medicine specialist or transfer to Level III perinatal facilities in accordance with ACOG guidelines and the Illinois Perinatal Act requirements for referral and/or transfer of high-risk women. Risk appropriate care will be ongoing during the perinatal period.
Postpartum Care
- Immediate And Subsequent Postpartum Visits, in accordance with the Department’s approved schedule, to assess and provide education on areas such as perineum care, breastfeeding/feeding practices, nutrition, exercise, immunization, sexual activity, effective family planning, pregnancy intervals, physical activity, SIDS, and the importance of ongoing well woman care, and referral to parenting classes, text4baby and WIC.
- Postpartum Depression Screening during the one-year period after delivery to identify high risk mothers who have an acute or long-term history of depression, using an HFS-approved screening tool.
- After delivery and discharge, the Enrollee will have a mechanism to readily communicate with her health team and not be limited to a single “six week” postpartum visit. Enrollees will be engaged in health promotion and chronic disease maintenance through the postpartum mother with Seamless Referrals to avoid interruption of care.
- Enrollees will be transitioned to the medical home for ongoing Well Woman Care. Enrollees who delivered and who are at risk of or diagnosed with diabetes, hypertension, heart disease, depression, substance use, obesity or renal disease will be identified and followed closely after the postpartum period.
- Interconception care management: Provide or arrange for interconception care management services for these high-risk women for 24 months following delivery.
Well Woman Exam
Well Woman Exam
- Preventive Well Woman Care: Provide evidence-based annual preventive well woman care to female Enrollees. At a minimum, the Plan will provide and document the following:
- Preconception and interconception care and reproductive life planning.
- The annual exam should include screening, counseling, evaluation, education, and immunizations based on age.
- The examination may vary but at minimum should include the following: routine vital signs, body mass index, palpation of abdominal and inguinal lymph nodes, and visual inspection of breast and genital.
- The components of the exam are based on Enrollee’s age, medical history, symptoms, and provider findings.
- Age-Appropriate Discussions: Exams will include age-appropriate discussions and anticipatory guidance related to reproductive health issues. Education will include, but not be limited to chronic disease management, breastfeeding reinforcement, reproductive life planning, and emphasis on the most effective method of family planning, specifically intrauterine devices, or the implant.
- Appropriate Referrals should be made to support services including WIC, interconception care management and parenting classes.
- Pelvic Exam: A pelvic examination is an appropriate component of a comprehensive evaluation of any patient who reports or exhibits symptoms suggestive of female genital tract, pelvic, urologic, or rectal problems. A routine pelvic exam is not required for members less than 21 years of age unless there is a clinical indication.
- Cervical Cytology Screening every three years from 21 years of age regardless of sexual debut and every 3-5 years after 29 years of age.
Clinical Breast Examination: Annual clinical breast examination for women aged 40 years and older; and in women aged 20-39 years, every 1-3 years
For Questions, please email CountyCare’s Quality Department at Q[email protected]
Care Coordination Resources
Pharmacy and Preferred Drug List
CountyCare maintains a Preferred Drug List (PDL), the same PDL as HealthChoice Illinois and all Medicaid Health Plans in Illinois. See our FAQs here.
View CountyCare PDL
Access the full Preferred Drug List
Formulary Search Tool
Check drug coverage online
MED Calculator
Calculate morphine equivalent doses
CountyCare works with CVS Caremark to administer pharmacy benefits, including the pharmacy prior authorization process. CountyCare requires prior authorization for select drugs on the PDL as well as ALL drugs not on the PDL. The PDL indicates which drugs require prior authorization. Most specialty drugs are not on the PDL and require prior authorization as described below.
Follow these steps for efficient processing of your pharmacy prior authorization requests:
- Complete and submit the online Medication Request Form or fax the printed Caremark Medication Request Form or Universal PA Form to 1-866-255-7569. Include detailed clinical information that will help CVS Caremark understand the need for the drug being requested.
- Fax to CVS Caremark at 1-866-255-7569.
- Once approved, CVS Caremark notifies the prescriber by fax and member by letter.
- For urgent or after-hours requests, a pharmacy can provide up to a 72-hour supply of most medications by calling the CVS Caremark Pharmacy Help Desk at: 1-800-364-6331.
- All pharmacy prior authorization requests for CountyCare members should be submitted to CVS Caremark.
Pharmacy Support
Email: [email protected]
Pharmacy Help Desk: 1-833-845-4702 (available 24 hours a day, 7 days a week)
Member Services: 312-864-8200
(Please have members contact CountyCare Member Services with their pharmacy-related questions.)
Rights & Responsibilities
CountyCare is committed to improving not just our members’ health but also provider satisfaction. To do this, we have established rights and responsibilities for both members and providers. Providers and members can apply their rights without any action taken against them.
If you believe your rights, or the rights of a CountyCare member were violated, please call Provider Services at 312-864-8200 / 855-444-1661 (toll-free)/ 711 (TTD/TTY).
To read more about your rights and responsibilities as a CountyCare provider
Eligibility Verification
Providers must verify a member’s eligibility on each date of service.
Methods to Verify Member Eligibility
- Online: To log on to the secure provider portal where you can check member eligibility Click Here.
- Automated Phone Line: Call our touch-tone automated member eligibility interactive voice response (IVR) system. Call 312-864-8200 / 855-444-1661 (toll-free)/ 711 (TDD/TTY) from any touch-tone phone and follow the appropriate menu options to reach our automated member eligibility-verification system 24 hours a day.
- Calling CountyCare Provider Services: If you cannot confirm a member’s eligibility using the methods above, call us at 312-864-8200 / 855-444-1661 (toll-free)/ 711 (TDD/TTY).
- Medi: Providers can also verify eligibility through the state of Illinois’ MEDI system online at myhfs.illinois.gov.
*Note that while PCPs are able to access their monthly member panel list through the provider portal, panel lists should not be used to determine eligibility for benefits. Member eligibility can vary in a given month. Please use one of the methods described above to verify member eligibility on the date of service.
Additional Eligibility Information
CountyCare members may also qualify for home and community-based waiver services (HCBS), supportive living facility (SLF), or long-term care (LTC). The state of Illinois determines eligibility for these programs. To confirm if a member is eligible for these services, contact CountyCare’s Provider Services at 312-864-8200 / 855-444-1661 (toll-free) / 711 (TDD/TTY).
Provider Resources
Training Materials
Prior Authorization
IL Association of Medicaid Health Plans (IAMHP) Billing Resources
Clinical
- HEDIS Measure Reference Guide
- Find Your Member’s Care Coordinator
- HCBS Member Communication Form
- LASIK Evaluation | Spanish | Polish
- Mammography Sites
- Neonatal Utilization Management FAQs
- Pay-for-Performance
- Quality of Care Referral
- Quality Assessment and Performance Improvement (QAPI) Program
- Youth in Care Psychotropic Medication Frequently Asked Questions
Transportation
- Transportation Billing Guidelines
- Transportation Information and Forms
Durable Medical Equipment
- Binaural Hearing Air Questionnaire
- C-PAP/BPAP Renewal Questionnaire
- Certificate of Medical Necessity for Continuation of External Insulin Infusion Pump Rental
- External Defibrillator Prior Approval Criteria
- Hospital Bed Questionnaire
- Knee Brace Questionnaire
- Motorized Wheelchair Evaluation Form
- Questionnaire for Airway Clearance Device
- Questionnaire and Order For Cranial Remolding Orthosis or Cranial Cervical Orthosis Congenital Torticollis Type
- Questionnaire for Enteral Nutrition
- Questionnaire For Negative Pressure Wound Therapy
- Questionnaire for Orthosis
- Questionnaire for Prosthesis
- Questionnaire For Tens Unit
- Wound Measurement Assessment Form
- Critical Incident Reporting Form
Newsletter & Notices
Health, Safety, Welfare, Reporting and Follow-up of Incidents
Health, Safety, Welfare, Reporting and Follow-up of Incidents
Incidents
Incidents regarding member health, safety and welfare are defined by Illinois state law. They involve actions that may risk the health, safety, and well-being of vulnerable adults by causing harm or creating a serious risk of harm to a person by their caregiver or other trusted person, whether or not harm is intentional.
Types of Incidents include:
- Physical abuse – the willful infliction of physical pain or injury, or the willful deprivation of services necessary to the physical safety of an individual
- Emotional abuse – an act that inflicts emotional harm, invokes fear or shame or otherwise negatively impacts the mental health or safety of an individual
- Neglect – the failure of an agency, facility, employee, or caregiver to provide important services needed to maintain the physical and or mental health of a vulnerable adult
- Financial abuse – the misuse or taking of the vulnerable adult’s property or resource using undue influence, breach of a fiduciary relationship, deception, harassment, criminal coercion, theft, or other unlawful or improper means
Incident Reporting Requirements
Incidents involving member abuse, neglect and financial exploitation must be reported to the appropriate authorities, as required by state law.
How to Report an Incident
Incidents related to CountyCare members can be reported to CountyCare by phone, fax, or email. You should use this form.
Call: 312-864-8200 / 855-444-1661 / 711 TTD/TTY
Fax: 312-637-8312
Email: [email protected]
You may also report Incidents to the right state agency, as follows:
- For members 18-59 with a disability or 60 and older living in the community: Illinois Department on Aging-Adult Protective Services Hotline Telephone Number: 866-800-1409 (voice)TTY: 888-206-1327
- For members under the age of 18 years old: Illinois Department of Children & Family Services (DCFS) Hotline Telephone Number: 800-252-2873 (voice)TTY: 800-358-5117. For non-DCFS membership.
- For members in Nursing Facilities: Department of Public Health Nursing Home Complaint Hotline Telephone Number: 800-252-4343
- For members 18-59 receiving mental health or Developmental Disability services in DHS operated, licensed, certified or funded programs: Illinois Department of Human Services Office of the Inspector General Telephone Number: 800-368-1463 (voice and TTY)
- For members in Supportive Living Facilities: Department of Healthcare and Family Services SLF Complaint Hotline Telephone Number: 800-226-0768
If you or a family member witness, told of, or suspect an incident of abuse, neglect, financial abuse or any other event that may place the member at risk or the member services at risk it is important to report the allegation immediately. Below are a few examples:
Physical abuse signs to look for
- Punching, hitting, beating
- Slapping, smacking
- Pushing, shoving, shaking
- Pinching, cutting, slicing
- Improperly physically restraining
Sexual abuse signs to look for:
- Rape
- Date rape
- Attempted rape
- Inappropriate touching
- Sexual assault or battery
- Coerced nudity
- Sexually explicit content
Emotional abuse signs to look for:
- Name calling
- Yelling, bullying
- Ridicule, insults
- Threats
- Coercion, manipulation
Neglect signs to look for:
- Injury that has not been cared for properly
- Dehydration or malnutrition without illness-related cause
- Poor coloration, sunken eyes or cheeks
Soiled clothing or bed - Lack of necessities such as food, water, or utilities Same clothing all of the time
- Fleas, lice on individual
- Unkempt, dirty
- Hair matted, tangled or uncombed
Financial abuse signs to look for:
- Accessing another individual’s funds without consent
- Changing ownership of assets
- Forged signature for financial transactions
- Changing legal documents, such as wills
- Using someone else’s money for personal reasons
Program Integrity (Fraud, Waste, Abuse, Mismanagement and Misconduct)
Program Integrity (Fraud, Waste, Abuse, Mismanagement and Misconduct)
CountyCare takes the detection, investigation, and prosecution of fraud, waste, abuse, mismanagement and misconduct very seriously. CountyCare’s Program Integrity efforts operate under policies, procedures and guidelines to ensure compliance with all Illinois and federal laws and regulations.
CountyCare’s Program Integrity efforts include performing front and back end audits to ensure provider compliance with billing regulations.
A Special Investigation Unit (SIU) performs routine internal monitoring and back end auditing of program integrity compliance risks and investigations of any issues identified. CountyCare promptly responds to compliance issues detected, including the correction of issues through education and the implementation of corrective action plans in compliance with program integrity-related requirements. In some cases, this may result in taking the appropriate actions against those who, individually or as a practice, commit fraud, waste, abuse, mismanagement or misconduct , including but not limited to:
- Remedial education and/or training to attempt to eliminate the egregious action
- Increasingly stringent utilization review process
- Recoupment of previously paid monies from a provider/practice
- Termination of provider agreement or other contractual arrangements
- Civil and/or criminal prosecution
- Any other remedies available to rectify the issue identified
The CountyCare SIU may also conduct prepayment reviews of provider claims as a result of suspected fraud, waste, abuse, mismanagement or misconduct, which may require the provider to submit additional records or documentation.
Some of the most common fraud, waste, abuse, mismanagement or misconduct issues identified are:
- Unbundling of codes
- Up-coding
- Add-on codes without primary CPT
- Diagnosis and/or procedure code not consistent with the member’s age/gender
- Use of exclusion codes
- Excessive use of units
- Misuse of benefits
- Claims for services not rendered
- Claims for services not covered
If you suspect or witness a provider inappropriately billing for Medicaid services or a member receiving inappropriate services, please call our anonymous and confidential hotline at 844-509-4669.
For more information on CountyCare’s Program Integrity process and efforts, please see the Provider Manual.
For more information on the False Claims Act and other federal and state laws including administrative, civil and criminal remedies for false claims and statements, and whistleblower protections with respect to the role of such laws in preventing and detecting fraud, waste, abuse, mismanagement, and misconduct in federal healthcare programs, please see the Cook County Health FWA Policy.
CountyCare expects that its providers will cooperate with all appropriate federal and state agencies in the detection and prevention of fraud, waste, abuse mismanagement and misconduct, as well as all investigations or prosecution by any duly authorized agency.
Provider Complaints, Disputes, Member Grievances, and Member Appeals
Provider Complaints, Disputes, Member Grievances, and Member Appeals
CountyCare has established a system to allow members and providers to bring their concerns to our attention. See below for additional information on provider complaints, member grievances and member appeals.
Provider Complaints
CountyCare has established a provider complaint system that allows a provider to dispute the policies, procedures, or any aspect of the administrative function. We take all complaints very seriously, and all provider complaints will be thoroughly investigated. CountyCare has designated a Provider Complaints Coordinator (PCC) to process these provider complaints. The PCC will provide written notice of resolution to the provider within thirty days from the decision date.
Provider Complaints may be submitted in writing to:
CountyCare Health Plan
P.O. Box 21153
Eagan, MN 55121
Or you can call Provider Services at 312-864-8200 / 855-444-1661 (toll-free) / 711 (TTD/TTY).
Communication with Care Coordination
Communication and collaboration between HCBS Waiver Providers and Care Coordination is essential to ensuring the health, safety, and welfare of CountyCare’s HCBS members.
Please utilize the HCBS Member Communication Form to communicate member needs, changes, and issues to ensure they are addressed timely, including:
- Start Date of Services
- When services need to be placed on hold, with the date and reason
- When services are resumed
- Changes in Member’s Living Situation (provide new address/phone if applicable)
- Changes in Member’s Condition and/or Circumstances
- Member’s Refusal or Non-Cooperation with Services
The HCBS Member Communication Form should be sent to [email protected].
Provider Notices and Newsletters
Providers in the CountyCare network can access notifications, Town Hall presentations, newsletters and other notices specific to providers here. Click on any of the PDFs below to view and download.
You can contact our Provider Services Team at [email protected].